Learn how to treat elbow pain associated with tight muscles and sore tendons, often the result of muscle imbalance and/or overtraining of pull-up movements. Pain near the medial epicondyle is commonly called “golfer’s elbow” or climber’s elbow. (Updated in 2021 and 2025 — originally posted in February 2015.)
Pain near the medial epicondyle is commonly called “golfer’s elbow” or “climber’s elbow”. Pain develops in the tendons connecting the pronator teres muscle and/or the many forearm flexors (responsible for finger flexion) to the knobby, medial epicondyle of the inside elbow.
In many cases medial tendinosis is a gradual-onset overuse injury due to climbing and training too often, too hard, and, most important, with too little rest. Furthermore, developing forearm muscle imbalance and muscle adhesion (trigger point) often contribute to elbow pain and exacerbate injury.
Before we dig deeper, I must point out that there are a number of less common injuries that can cause elbow pain and mimic climber’s elbow (misdiagnosis is not uncommon). If your elbow pain is significant and/or getting worse, I strongly recommend visiting a doctor versed in climbing injuries. Here’s a link to an excellent book on climbing injuries, Dr. Volker Schöffl’s One Move Too Many.

Anatomy Overview
Consider that the muscles that produce finger flexion are anchored on or near the medial epicondyle. Furthermore, the muscles that produce hand pronation (that turn the palm outward to face the rock) originate from the medial epicondyle.
Biceps contraction produces supination (turning of the palm upward), but in gripping the rock you generally need to maintain a pronated, palms-out “pull-up” position. This battle, between the supinating action of the biceps pulling and the necessity to maintain a pronated hand position (to maintain grip with the rock), strains the pronator teres muscle and its attachment at the medial epicondyle.
Given the above factors, it’s easy to see why the tendons attaching to the medial epicondyle are subjected to sustained stress and, inevitably, develop microtrauma. Just as muscular microtrauma is repaired to new level of capability, tendons increase in strength and can withstand higher stress loads given adequate rest. Unfortunately, the repair and strengthening process occurs more slowly in tendons than in muscles. Eventually, the muscles are able to create more force than the tendons can adapt to—the result is painful tendinopathy (tendinosis).
Treatment and Rehab
As in treating other injuries, you can more easily manage tendinopathy (or any connective tissue injury) and speed your return to climbing by early recognition of the symptoms and proactive treatment. The mature and prudent approach of attending to the injury early-on versus trying to “climbing through it” could mean the difference between six weeks and six months (or more) of climbing downtime.
Treatment of tendinosis and tendinitis has two phases: Phase I involves steps to relieve pain and reduce inflammation (in the case of tendinitis); Phase II is engaging in rehabilitative and stretching exercises to promote correct alignment of collagen tissue and prevent recurrence.
Phase I demands withdrawal from climbing (and intensive sport-specific training) and commencement of pain-reducing and anti-inflammatory measures. Icing the elbow for twenty minutes, three to six times a day, and use of NSAIDs will help reduce inflammation and pain following injury. Cease ice and NSAID use within a few days to a week, and begin appropriate rehab exercises to lightly load the tendons.
Note: A cortisone or PRP injection may be helpful in chronic or severe cases, although this practice is somewhat controversial among physicians. Two newer procedures, Extracorporeal Shockwave therapy and TENEX, have yielded promising results—look into these for treating chronic cases of tendinosis.

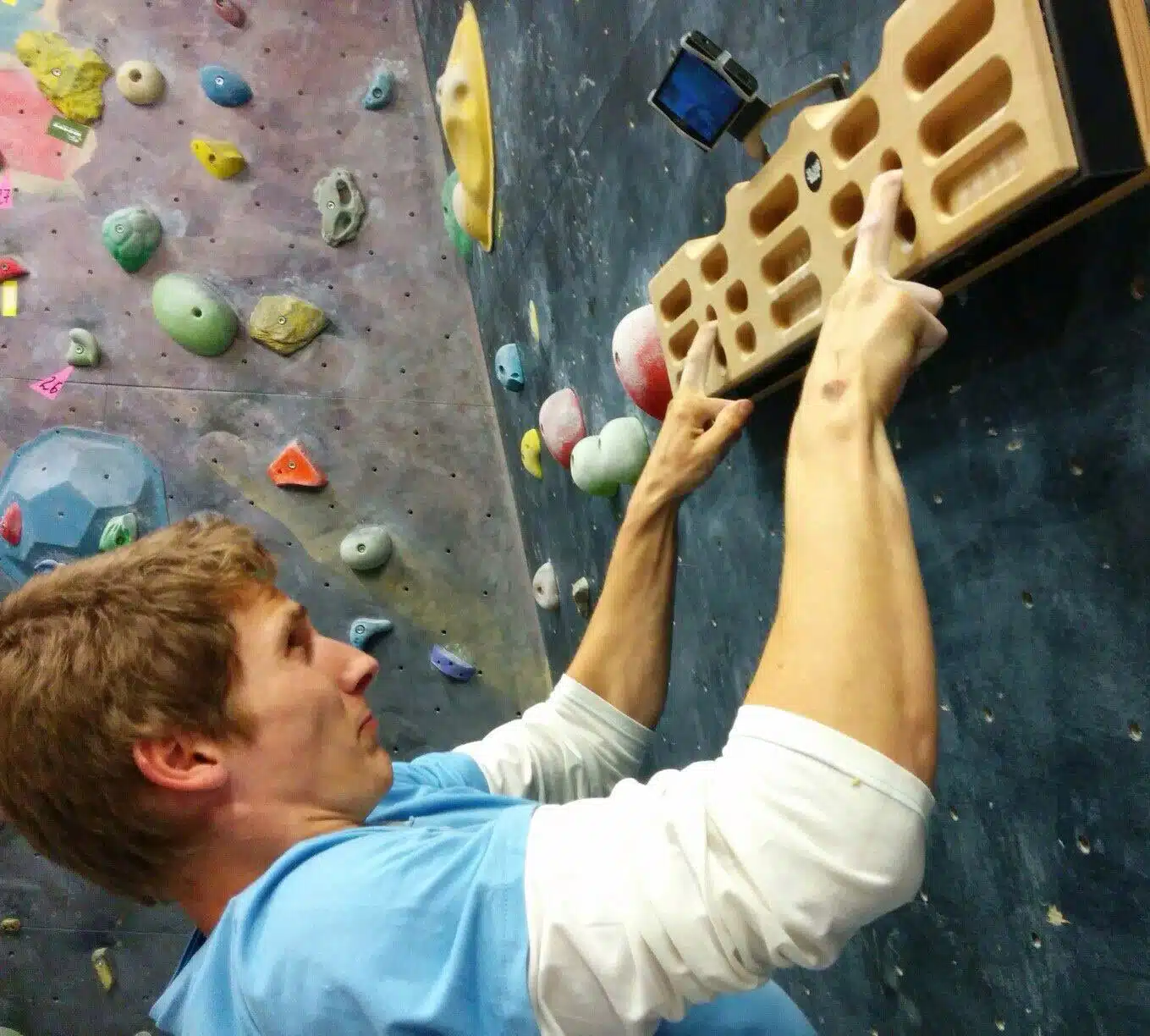
Isometric hang with neutral grip.
The goal of Phase II is to retrain and rehabilitate the injured tissues through use of mild stretching and strength-training exercises. Appropriately loading the tendons is essential to stimulate collagen synthesis—isometric and slow eccentric exercises are ideal.
Since forearm-muscle imbalance plays a role in many elbow injuries, it’s vital to perform exercises that strengthen the weaker aspects of the forearm—hand pronation for medial tendinosis and hand/wrist extension for lateral tendinosis (pain near the outside/lateral bony aspect of the elbow, and the topic of a separate article).
Although some dull pain is likely during this rehab phase, avoid any exercise or activity that causes sharper pain or lingering (or worsening pain) after a workout. Conventional pull-ups, fingerboard training, campus training, and the like are often problematic and should only be done in small doses, if at all, until the condition has resolved.
Rehab/Prehab Exercises
Always begin rehab and training sessions with some warm-up activities, both generalized and specific. Stretch twice daily the finger flexor, extensor, and pronator muscles (see photos below). Once the stretching exercises have successfully restored normal range of motion with no pain, you can introduce strength training with the forearm pronator exercise (below). It’s important to progress slowly with training exercises and to cut back at the first sign of anything more than slight pain.

Low-load isometric finger flexor training with blood flow restriction straps.
Two more helpful exercises to help accelerate recovery are lock-off hangs with neutral grip and blood flow restriction training. Perform two or three 15- to 20-second mid-range-of-motion lock-offs with a neutral grip (photo). These “density hangs” impart a beneficial stress-relaxation of the injured tendon and provide a signal for proper collagen remodeling. You may be able to further aid healing by engaging in some low-load blood flow restriction training.
Return to Climbing
After three to four weeks of rehab/training, begin a gradual return to climbing. Start with easy vertical routes, and take a month or two to return to your original level of climbing. Continue with the stretching and strength-training exercises indefinitely—as long as you are a climber, you must engage in these preventive measures. Failed rehabilitation and relapse into chronic pain may eventually lead to a need for surgical intervention.
Counterforce Bracing and Taping
A counterforce brace designed specifically for tennis elbow tendinosis can provide some comfort by dispersing forces away from the underlying tissues. More beneficial for climber’s elbow, however, may be a narrow tape band passing snugly around the upper forearm (just distal to the medial epicondyle). Important: These braces are not a substitute for proper rehabilitation; however they may be somewhat protective during the return to climbing.
Rehab/Prehab Stretches & Exercises
Twice or thrice daily stretching is essential. Be sure to target both the flexors and extensors using the two exercises below.
The flexor stretch targets the muscles and tendons that apply force to the medial epicondyle, so this stretch may yield a slight dull pain (okay). In a standing position, bring your arms together in front of your waist. Straighten the arm to be stretched and lay the fingertips into the palm of your other hand. Position the hand of your stretch arm so that the palm is facing down with the thumb pointing inward. Pull back on the fingers of your straight arm until a mild stretch begins in the forearm muscles. Hold this stretch for about twenty seconds.
Now, release the stretch and turn the hand 180 degrees so that your stretch arm is now positioned with the palm facing outward and the thumb pointing out to the side. Using your other hand, pull your fingers back until a stretch begins in the forearm muscles. Hold for ten to twenty seconds. Repeat this stretch, in both positions, with your other arm. Finish up with a minute of self-massage to the forearm flexor muscles using deep cross-fiber friction.

Finger & Wrist Flexor Stretch

Extensor Stretch.
The extensor stretch is important, yet often overlooked. It targets the muscles of the lateral forearm as well as the commonly sore and tight brachioradialis muscle. These muscles are especially strained when crimping with a chicken-winged arm position, and so daily stretching (and use of an Armaid) is helpful for lengthening the tissues and releasing tension that can eventually contribute to lateral tendinosis.
With nearly straight arms, cross your hands in front of your body and interlace your fingers, palms together. While maintaining mild tension throughout the length of both arms, pull with one hand to flex the wrist of the other hand until you feel the stretch develop in the finger/wrist extensors along the outside of the forearm. Hold the stretch for about twenty seconds and then pull with the other hand to create a stretch along the other arm. Perform the stretch two or three times stretching each way/arm. This is a good stretch to do every day, whether you’re at work, home, then gym, or the crags. Just do it!

Pronator Teres Exercise – Start (left) and Finish (right).
This pronation exercise targets the small, but important pronator teres muscle that often contributes to elbow pain and some cases of tendinosis. Sit on a chair or bench with your forearm resting on your thigh with the hand in the palms-up position. Firmly grip a sledgehammer with the heavy end extending to the side and the handle parallel to the floor. Turn your hand inward (pronation) to lift the hammer to the vertical position. Stop here.
Now, slowly lower the hammer back to the starting position–slowly count to five as you perform the lowering (eccentric) phase. Stop at the horizontal position for one second before beginning the next repetition. Continue lifting the hammer in this way for fifteen to twenty repetitions with the emphasis remaining on a slow eccentric (lowering) phase throughout. Choke up/down on the hammer to adjust the resistance/difficult. Perform two sets with each hand.
Note: When used as a rehab exercise, it’s best to do only the lowering phase—use your free hand to assist in returning the hammer to the top position. Read more about rehab/prehab training of the climbing antagonist muscles here >>
Finally, don’t forget to include the lock-off “density” hangs and some blood flow restriction training as described above. Disciplined use of the five exercises and stretches detailed in this article will resolve most minor cases of medial tendinosis (climber’s elbow) in a month or two.
Summary Tips for Treating Elbow Tendinosis
- Cease climbing and climbing-specific training. Avoid any exercises or movements that provoke/incite the elbow pain.
- Apply ice to the injured area and take NSAID medications only if the injury produces acute pain or palpable swelling (most elbow tendinopathy does not). Cease use of ice and NSAIDs as soon as swelling and pain diminish—further use may slow healing.
- Never use NSAIDs to mask pain in order to continue climbing while injured. Regular use of NSAIDS (and smoking) may actually weaken tendons! Instead consider taking a natural anti-inflammatory pain relief supplement such as REDUX-HP
- If no swelling is present, begin mild stretching, light massage, and use of a heating pad (ten minutes) three times per day. Most important is twice-daily use of the forearm stretches shown above. Daily Armaid use may improve forearm muscle tissue quality, however, be sure to never use on the Armaid directly to tendons.
- Engage in rehabilitative exercises on an every-other-day basis. For medial elbow pain (climber’s elbow) use the pronator exercise, isometric lock-offs with a neutral grip, and some low-load blood flow restriction training. For lateral elbow pain (tennis elbow) train with reverse wrist curls, reverse arm curls (palms down on a curl bar),and some blood flow restriction training.
- Cautiously return to climbing when your elbow is pain-free and no sooner than after two to four weeks of strength-training exercise. Begin with easy, foot-oriented climbing for the first few weeks—focus on movement training and avoid hard, powerful arm movements. Cease climbing if you experience pain while climbing and immediately return to step 2.
- Commit to long-term training of the forearm pronator and extensor muscles, and enjoy daily stretching and Armaid use for as long as you are an active climber.
PRO TIP: Nourish Your Tendons and Joints Before Each Climbing Workout!
A growing body of research has demonstrated the benefits of a specific pre-exercise nutritional protocol designed to amplify collagen synthesis and soft tissue recovery. Consuming vitamin C-enriched hydrolyzed collagen before rigorous training is the lynchpin of the protocol shown to support connective tissue remodeling and recovery from powerful workouts. This is revolutionary information for a hard-training climber! Read more here >>
Copyright © 2000–2025 Eric J. Hörst | All Rights Reserved.